Why Health Care Costs Keep Rising—And What to Do About It
In this opinion column, a health policy expert offers a big-picture view on controlling health spending
When economist Charles Wheelan published an analysis titled “The Top 10 Reasons for Soaring Health-Care Costs,” it was refreshing to read about the problem from an economics point of view. What Wheelan did not cover, however, was what we can do to address the issues that continue to cause health care costs to spiral out of control. What follows is a point-by-point look at Wheelan’s top 10 reasons followed by a discussion of what we are doing—or could do—to control costs better.
Reason 1.
Nobody Shops for value
Wheelan argues that when it comes to health care, everyone wants and expects the best. “There's no medical equivalent of Wal-Mart,” he writes. “Everyone wants Neiman Marcus.”
Solution:Some health plans are addressing this issue by discouraging patients from using expensive facilities for common problems, such as a sore throat, through co-pay incentives and member education. Not only are patients encouraged to find a less expensive facility, they also are encouraged to ask the doctor to write generic prescriptions.
The question is, how do patients know which facilities offer reasonable prices and quality medical care? It will take greater health care cost and quality transparency—and better consumer education—to get health care shoppers to the same level of sophistication they use in buying other high-end goods (e.g., cars), but progress is being made. A number of health plans now offer cost information on various treatment options, and web sites such as HealthGrades offer quality information on doctors, making it possible for people to shop for health care online.
Reason 2.
Medical Innovations Are Usually More Expensive
The basis of medical progress is learning to do new things, no matter the cost. In the case of pharmaceuticals, the system has been designed so new drugs are expensive. Breakthrough medications receive patent protection, and the better the drug, the more its producer can charge. High prices yield high profits, which creates an incentive to develop the next generation of drugs.
Solution:Although we, as a society, have agreed to pay more for innovative medications and medical devices, especially those that introduce new cures, we have not agreed on who is going to pay for them. Part of the solution lies in the expansion of employer-sponsored wellness and health promotion programs that focus on keeping healthy people healthy and helping those who are sick to better manage their illnesses by steering them toward proven treatments. value-based benefit plan design tries to achieve this by removing barriers that may be barring patient access to the most effective medications.
Furthermore, not all innovations (which include diagnostic tests, imaging tests, medications and medical devices) should be treated equally. While some add value, some do not. One solution is to use a creative plan design that identifies the most effective innovations and reimburses them with a premium.
Reason 3.
Some Health Care Is a ‘Luxury Good’
Used as a technical economic term, a “luxury good” is something wealthy people demand in disproportionately greater amounts than less wealthy people do. Richer societies and richer people within a society have higher expectations for health care. They expect medical fixes—such as hip replacements, stomach stapling and Lasik eye surgery—for problems that people with lower expectations will just tolerate.
Solution:While it’s easy to poke fun at medical tourism, it may well emerge as one of the solutions to this problem. Medical tourism generally involves traveling to another country for non-emergency care, including knee replacements, shoulder surgery and even heart bypasses. A knee or hip replacement that may have a retail price of $65,000 to $80,000 in the United States costs between $8,000 and $10,000 in India. The Deloitte Center for Health Solutions predicts that the number of Americans using medical tourism could jump tenfold over the next decade, to nearly 16 million a year.
Reason 4.
We Don’t Pay for What We Consume
Health care is unique in that neither the service provider nor the patient gets the bill, especially when insurance out-of-pocket maximum provisions are reached. The patient who is directly involved in the transaction has little incentive to control costs when out-of-pocket costs are removed. When insurance companies try to do so, it can lead to arbitrary limits on care, time-consuming hurdles for more expensive procedures and additional bureaucracy for doctors. Even then, it’s easy to game the system.
Solution:One possible solution is moving away from fee-for-service provider reimbursement and returning to a staff-model health maintenance organization (HMO), where providers employed by the health plans are charged with offering patients the most cost-efficient care without compromising quality. Two studies have found that this model works quite well. A 2002 paper in the British Medical Journal (BMJ), “Getting More for Their Dollar: A Comparison of the NHS with California’s Kaiser Permanente,” compared HMO provider Kaiser and Britain’s National Health System (NHS), concluding that Kaiser achieved better outcomes than the NHS for similar inputs. And a 2003 study in the BMJ, “Hospital Bed Utilization in the English NHS, Kaiser Permanente, and the US Medicare Program: Analysis of Routine Data,” which reported on hospital stay lengths, produced similar conclusions.
Over the past few years, several large employers have brought care delivery on-site in the form of clinics, using the same premise as the staff-model HMO. Revisiting global provider payments per admission or bundled payments for treating all the medical needs of specific patients with chronic disease might return to favor.
Reason 5.
Baumol's ‘Disease’
Not a disease, but an important insight by economist William Baumol on what afflicts certain sectors of the economy, such as health care and higher education. He found that as societies become richer, labor-intensive endeavors, such as health care, become increasingly expensive relative to goods and services that can be produced using less labor. As long as the doctor-patient relationship remains relatively unchanged, health care costs will rise faster than prices in general.
Solution:Because there are no economies of scale, a surgeon cannot perform more than X number of surgeries and a primary care physician cannot see more than X number of patients in a day (although we have seen the latter rise dramatically in the past two decades). For them to keep up with others, who are earning more money in less time because of technological advances, they have to increase their unit cost.
Pay-for-performance-type programs can help identify providers who are practicing quality medicine in the most judicious and cost-effective way. Once such high-quality and cost-efficient providers are identified, patients need to be directed to them. Specialized cancer and transplant centers are a good example of where upfront costs are relatively high but long-term outcomes are better and repeat illnesses are fewer.
Reasons 6 & 7.
Living Longer and Living an Unhealthy Lifestyle
Not only are people living longer (which in itself increases health care costs), but too many people are living unhealthy lives. This includes smoking, eating fast food and driving instead of walking, to name but a few.
Solution:While we can’t change the fact that people are living longer (nor would we want to), we can help them live healthier lives. The latest shift in health care is to focus on keeping the healthy healthy and to stop diseases from progressing from bad to worse. This can be achieved through wellness and health promotions, health education and coaching, communicating information on healthy lifestyle choices, and making sure those who need care have access to the right care at the right time to maximize clinical and economic value. People who are at risk or at high risk can be identified via health risk appraisals and sophisticated technology and tools, such as predictive modeling, which uses claims data to identify risk.
Reason 8.
The Uninsured
The uninsured end up costing the system a great deal of money. In a family that is uninsured, a child with a high fever and a bad cough will probably be treated in a hospital emergency room—a very expensive use of a trauma center and its highly trained staff. Or the child might not be treated at all until five years later when he or she develops asthma or another chronic condition that could have been managed far less expensively with better primary care.
Solution:This is a problem that needs government intervention. Although President Barack Obama has pledged to intervene, his health care program has yet to be addressed—specifically, how his programs will cover all Americans in the most cost-effective delivery setting.
One solution that plan sponsors can undertake in the meantime involves helping their pre-age-65 retirees with health insurance. They can take advantage of the innovative solutions that some health plans now offer—allowing employees to prefund premiums that contribute toward buying coverage after retirement but before they are eligible for Medicare.
Reason 9.
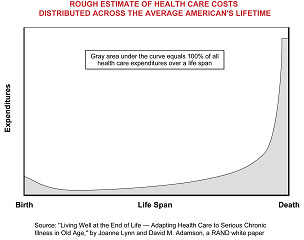
The High Cost of End-of-Life Care
Even people who are treated successfully for heart disease or cancer eventually die. Any medical success begets additional medical expense, which is especially true for end-of-life care. The last six months of life are typically the most expensive period of a person’s life (see the chart below).
The escalating cost of treating illness at the end of life raises moral and politically charged issues that are difficult to address: What is the actual value of using expensive treatments on people whose life expectancy is drastically limited, even with the treatment? While other countries have begun to base coverage decisions, in part, on how many years of quality life a treatment is expected to produce—for example, the clinical guidelines created by the U.K.’s National Institute for Clinical Excellence—this issue still seems to be taboo in the United States. Most of these costs are incurred by Medicare and Medicaid.
Solution:We need to be better at considering quality of life in decisions about treatments and services for chronically ill elderly patients. It has been suggested that Medicare and Medicaid could form a governing body of clinicians that can make and authorize these difficult decisions.
In addition, society needs to make better use of hospice care. Employers and plan sponsors should educate their beneficiaries about hospices and the situations in which they are the best option.
Reason 10.
Malpractice Suits
Malpractice is more of a legal problem than an economic one because doctors tend to practice “defensive medicine” out of fear of being sued. Seeking to avoid lawsuits, they have an incentive to over-treat all kinds of maladies. Research shows that physicians in countries such as the United States—where the risk of malpractice suits is high—tend to order more investigative tests than those in countries with less risk, such as the U.K. (See, for example, the New York Times article “Why Does U.S. Health Care Cost So Much?”)
Solution:Washington Post columnist George F. Will has proposed an appropriate solution to this complex issue. We have juries of people who have no knowledge of the complexities of medicine handling decisions on whether a patient’s death resulted from negligence on the part of the physician or whether the doctor did everything in his or her power to save the patient. Instead, the state judicial system could create a panel of highly qualified judges with access to independent clinicians who are familiar with the highly complicated nature of such cases and remove some of the emotional overreactions by juries that result in disproportional monetary awards that should be reserved for cases of gross negligence. This will help physicians use sound clinical judgment instead of practicing defensive medicine.
One More Reason: Lack of Access to Complete Information
Doctors collect and create a lot of information—everything from notes to diagnosis codes. The insurance companies add another level of data. While much of this information could be used to improve treatment and reduce costs, no one is in a position to see it all. A doctor who prescribes a treatment doesn’t know what it costs or whether the patient’s insurance covers it. An insurance company that questions a doctor about a treatment might never receive all of the information it needs. When a patient switches providers, it can result in duplicate tests and services and potentially dangerous treatments. All this creates tremendous administrative waste and resource consumption for providers and payers.
Solution:Electronic medical records (EMR) and health information exchange (HIE) are two steps in the right direction toward health care interoperability (the ability of different information technology systems and software applications to communicate; to exchange data accurately, effectively and consistently; and to use the information that has been exchanged). Developing standards for EMR interoperability is at the forefront of the president’s health care agenda. Many physicians have computerized practice management systems that can be used in conjunction with HIE, allowing them to share patient information (e.g.,lab results, public health reporting), which is necessary for timely, patient-centered and portable care.
Similar movement is happening on the payer side, which is attempting to collect more information from providers as well as consumers. They are making decision-support tools available to their beneficiaries, to help them navigate the system. Some payers are also adopting personal health records, which members can take with them if they change insurance providers.
Another step in the right direction is the patient-centric medical home model, in which a patient’s physician knows everything there is to know about that person’s health care. This requires comprehensive patient management software that allows the physician to coordinate all the care the patient needs.
Conclusion
The good news is, there are potential solutions to most of the reasons health care is so expensive. The real challenge is in getting the different stakeholders to work together to work together to solve this monumental problem.
Sadhna Paralkar, M.D., is a health management consultant to The Segal Co. Her areas of expertise include health care informatics, medical management program design, clinical operations, benefit plan design and network management strategies to optimize health improvement while containing costs.
Was this resource helpful?
Validate your HR expertise
Earning your SHRM-CP credential makes you a recognized expert and leader in the HR field.
Related Content

Learn how Marsh McLennan successfully boosts staff well-being with digital tools, improving productivity and work satisfaction for more than 20,000 employees.

The proliferation of artificial intelligence in the workplace, and the ensuing expected increase in productivity and efficiency, could help usher in the four-day workweek, some experts predict.

As artificial intelligence technology continues to develop, the demand for workers with the ability to work alongside and manage AI systems will increase. This means that workers who are not able to adapt and learn these new skills will be left behind in the job market.